(HRH_STAFF_NAT) Number of health workers who are working on any HIV-related activities (i.e., prevention, treatment and other HIV support) based out of PEPFAR-supported facility sites
Export Indicator
This indicator is the total number of staff working on HIV based out of PEPFAR facility sites. This includes staff engaged in community work, but who are supported and based out of a PEPFAR supported facility. This includes but is not limited to Community Health Workers (CHWs) engaged in outreach, ARV delivery, or working as Linkage Officers, Peer Navigators, or Adherence Group coordinators.
This is NOT a cumulative total, but a one-time count undertaken during the final quarter. Only filled staff positions at respective facility should be counted.
For this indicator, a “PEPFAR supported site” should include any facility site in the PEPFAR geographic organizational hierarchy list in DATIM, which also reported any site-level programmatic target or result during the same reporting period. Omit facilities which were previously supported by PEPFAR but were not assigned any targets nor reported any results for any program area during the same reporting period. Include all health care workers irrespective of whether any or all are receiving PEPFAR support (this is captured in HRH_CURR). We do NOT need any workers reported at the community level for this indicator; workers supported by the government or other organizations, but not based out of a PEPFAR supported facility should not be reported.
HIV/AIDS has placed significant demands on the already constrained health workforce in many low-income countries. The rapid scale-up of ART is placing additional demands on the health workforce.
In the majority of PEPFAR countries, there are overall shortages of HRH, particularly in rural and remote areas, leading to insufficient numbers of health workers according to internationally recommended levels (2.3 doctors, nurses, midwives/1,000 population). Many countries experience HRH shortages and/or imbalances by population densities (e.g., HRH shortages in rural areas) that are not related to population health needs, including HIV epidemiology. Addressing density, distribution, and overall utilization of HRH is important in increasing access to HIV services.
This indicator allows PEPFAR to analyze the availability of staff to provide HIV services at PEPFAR supported facilities. Data should be reviewed against site target achievement and investment. The first year of data collection will serve as an Integral benchmark for continued analysis.
Teams can also look at this indicator in conjunction with HRH_CURR that captures number of PEPFAR supported workers at PEPFAR-supported sites. This will allow PEPFAR to conduct analysis to determine if the number of PEPFAR-supported staff is appropriate vis- à-vis the number of other staff at the facility providing HIV services.
There is no universal benchmark against which to measure these data and no ideal PEPFAR to non-PEPFAR ratio. However, over time we would hope to see a decrease in the number of PEPFAR-supported staff. As this happens countries should carefully monitor any changes total number of staff working in HIV service delivery at sites and quality of services.
Number of health workers who are working on any HIV-related activities (i.e., prevention, treatment and other HIV support) based out of PEPFAR-supported facility sites
N/A
How to collect:
A “PEPFAR supported site” for the purpose of this indicator includes any facility site in the PEPFAR master facility list in DATIM which also reported any programmatic target or result during the same reporting period.
Report all HRH at those sites who are working in HIV-related activities, regardless of whether they are supported by PEPFAR or not.
PEPFAR team should collect and report on this data during the last quarter of the year. Ideally this data would come from a MoH HRIS/HRID system, or a payroll system from a Ministry of Finance.
Total number of health workers should be reported. Report HRH who are actively working on services or programs related to HIV at the time of data collection, not including staff who have resigned, absconded, are dismissed, are pending hiring, or are on extended leave (e.g., for graduate studies). Unfilled positions or vacancies should not be included.
If possible, avoid collecting data across a period which spans across a major budgetary change or a health worker graduation and placement period. The graphic below outlines the relationship between the HRH MER and host country indicators:
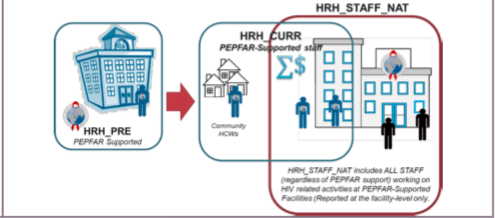
Reporting level: Report at all PEPFAR-supported site: This indicator is the number of occupied positions working on HIV based out of PEPFAR facility sites.
Reporting frequency: Annually
Indicator changes (MER 2.0 v2.3 to v2.4): Indicator has moved from being a standard MER indicator to host country reporting. Indicator should be reported by USG
Data entered by: This data should be entered in DATIM by the USG country team.
Guiding narrative questions:
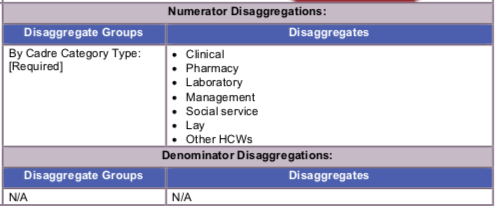
- For all categories of workers, including other, please provide description of specific cadres in the narrative when reporting.