(GEND_GBV) Number of people receiving post-gender-based violence (GBV) clinical care based on the minimum package
Export Indicator
This indicator measures delivery of a basic package of post-GBV clinical services (including PEP and EC). NOTE: This indicator DOES NOT include GBV Prevention activities or non-clinical community-based GBV response (e.g., shelter programs, case management).
This indicator will enable PEPFAR to:
- To determine the number of individuals that are suffering from GBV and reporting to clinical partners.
- To assess whether post-GBV clinical services are being used.
- Gain an understanding of the uptake of post-GBV clinical services offered across PEPFAR countries.
- Provide important information to key stakeholders about PEPFAR programs that mitigate women and girls’ and other marginalized populations’ vulnerability to HIV/AIDS.
- Support efforts to assess the impact of post-GBV clinical services by correlating the reach (i.e., number of people served) of these services over time with outcomes related to GBV (and HIV/AIDS), as described through other data collection efforts such as survey data (DHS/PHIA/VACS).
- Identify programmatic gaps by analyzing the number and ages of people receiving services, as well as the reach of services in particular geographic areas.
Number of people receiving post-gender-based violence (GBV) clinical care based on the minimum package
N/A
Data sources are standard program monitoring tools, such as forms, log books, spreadsheets and databases that national programs and /or partners develop or already use.
Data should be collected continuously at the point of service delivery (i.e., ANC, PMTCT, ART, etc.) and aggregated in time for PEPFAR reporting cycles.
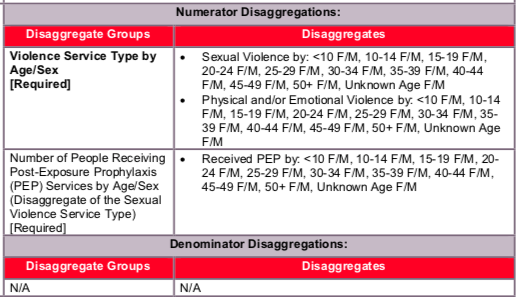
The indicator can be generated by counting the number of persons receiving post-GBV clinical care, disaggregated by the age group and sex of the client receiving the service, as well as the type of service (sexual violence or emotional/physical violence) and PEP provision (see below for disaggregation information).
To adequately capture the provision of these services, logs and monitoring forms will need to be used wherever the services are offered. These forms will need to track both the outcome of the initial assessment and the provision of referrals or services. For PEP specifically, registries should collect both the administration of the PEP as well as its completion and the patient’s adherence.
Special considerations: As outlined in the Program Guide for Integrating GBV Prevention and Response in PEPFAR Programs all programs seeking to address GBV must first and foremost protect the dignity, rights, and well-being of those at risk for, and survivors of, GBV. There are four fundamental principles for integrating a GBV response into existing programs and specific actions for putting these principles into practice. These principles are as follows:
How to review for data quality:
Numerator ≥ subtotal of each of the disaggregation: The number of people receiving post-GBV clinical care should be greater or equal to the sum of each individual disaggregate group.
Total sexual violence numerator ≥ PEP age/sex disaggregates for the same reporting period.
Reporting level
Facility & Community
- Provision of Clinical Services: (all of the following must be in place, including relevant commodities, and ability to count individuals—independent of whether individuals use the specific service)
- Rapid HIV testing with referral to care and treatment as appropriate
- Post exposure prophylaxis (PEP) for HIV -- if person reached within the first 72 hours
- STI screening/testing and treatment
- Emergency contraception, if person is reached in the first 120 hours. PEPFAR funds cannot be used to procure EC. EC is legal in all PEPFAR countries except Honduras, so should be available in all countries except for Honduras
- Counseling (other than counseling for testing, PEP, STI and EC)
- Provision of Clinical Services: (all the following must be in place and available to count persons—independent of whether people use the specific service)
- Rapid HIV testing with referral to care and treatment as appropriate (Please note that individuals should also be counted under the MER HIV testing and counseling indicator (i.e., # of individuals who received HIV testing and counseling services and received their results).
- STI screening/testing and treatment
- Counseling (other than for HIV counseling and testing)
- Longer-term psycho-social support (e.g., peer support groups)
- Legal counsel
- Police
- Child protection services
- Economic empowerment
This indicator DOES NOT include GBV prevention activities or non-clinical community-based GBV response.
N/A
Indicator changes (MER 2.0 v2.3 to v2.4): None
PEPFAR Support definition:
Standard definition of DSD and TA-SDI used.
Provision of key staff or commodities for GEND_GBV includes: ongoing procurement of commodities (e.g., ARVs, rapid HIV test kits, STI testing or treatment commodities) or funding of salaries (partial or full) for HCW actively delivering the components of GBV care in accordance with international or national protocols or guidelines [i.e., physicians, nurses, and other health care workers who can assess GBV and provide treatment and appropriate referrals.
Ongoing support for GEND_GBV service delivery improvement includes: mentoring and supportive supervision, training, guidance development, site level QA/QI, regular assistance with monitoring and evaluation functions and data quality assessments, or commodity consumption forecasting and supply management.
Guiding narrative questions:
- How are GBV cases identified in the community and/or at the facility? If cases are identified at the community, how are they referred to a facility for post-GBV clinical care?
- Of those coming in for services who are screened and disclose sexual violence, what proportion receive PEP? What proportion of those who disclose sexual violence refuse PEP?
- Is site level data on the type of violence disclosed collected? If so, please provide available data in the narratives on the proportion that disclose physical and/or emotional violence, and of those choose to receive services.
- What proportion of clients experienced both sexual and physical/emotional violence?
- Note: If clients experience both sexual and physical/emotional violence, they should only be counted under sexual violence to ensure that there is no duplication.