(CXCA_SCRN) (including CXCA_SCRN_POS) Percentage of HIV-positive women on ART screened for cervical cancer
Export Indicator
This indicator is vital for understanding and estimating the demand for screening services and forecasting and planning for the resources required to meet that demand and the resulting treatment needs. Disaggregation enhances sensitivity of this indicator in order to help identify the need for further outreach, as well as trigger further situational investigation at lower levels of the health system.
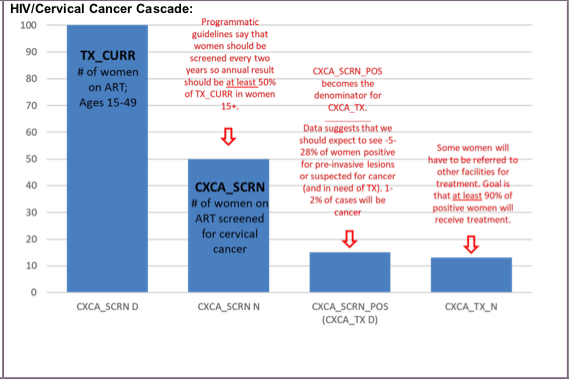
For VIA, the benchmark of 5%-25% screen-positivity for women (aged 30-60) screened for the first time should be used when monitoring performance. (WHO, 2013; ACCP, 2004)
Number of HIV-positive women on ART screened for cervical cancer
Number of HIV-positive women ages 15+ on ART at PEPFAR-supported sites
How to calculate annual total:
Sum results across reporting periods for the numerator. Denominator (TX_CURR) is a snapshot indicator.
How to collect:
The primary data sources for this indicator are registers or logbooks in use at the point of cervical cancer screening service delivery at PEPFAR supported ART sites. Client and facility level data collection tools should include the data elements required for disaggregation.
Data for the numerator should be generated by counting the total number of HIV-positive women on ART who received a cervical cancer screening test.
For the purposes of this indicator, “screened” is defined as receiving the tests necessary to determine the need for treatment of precancerous lesions – or referral for suspected invasive cervical cancer.
- For programs using a VIA based test-and-treat strategy, the number of women receiving a VIA result should be counted here.
- For programs using a test-triage-treat strategy (e.g., HPV test with VIA triage, with treatment only if the woman is VIA positive), the following should be counted:
- The number of women who received a negative result on the initial screening test (e.g., HPV test)
The number of women who received BOTH a positive result on the initial screening test (e.g., HPV test) AND either a positive (or suspected cancer) or negative result on the triage test (e.g., VIA) should be counted here.
Only completed screenings should be counted under this indicator – screening tests that were not completed due to cervicitis or other issue should not be counted. Screening visits where cancer is suspected based on initial speculum examination, prior to the application of acetic acid, should be counted as ‘completed screenings’. This is because the defined purpose of the screening was fulfilled (i.e., to identify individuals with increased probability of having either the disease itself or a precursor of the disease).
How to review for data quality:
The numerator for this indicator should not be larger than TX_CURR among women 15+.
Reporting level: Facility
Reporting frequency: Semi-annually
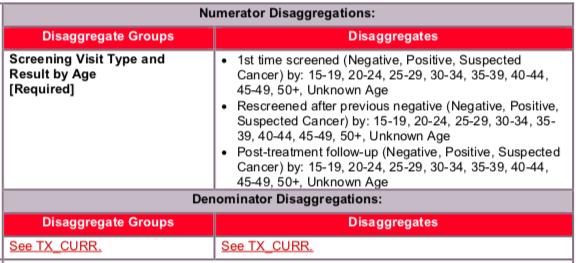
Disaggregate descriptions and definitions:
Result:
- Negative
- Indicates that neither a lesion, nor any indication of invasive cervical cancer were visualized during the VIA test.
- Positive (CXCA_SCRN_POS)
- Indicates the visualized presence of aceto-white lesion on the cervix following the application of acetic acid.
- In practice, women with a positive result are further differentiated into ‘eligible for cryotherapy’ and ‘ineligible for cryotherapy’, based on the size and location of the lesion.
- Women with fulminating masses or other indication of suspected cervical cancer are not counted under this disaggregate.
- Suspected cancer
- Indicates the visualized presence of a fulminating mass, or other clinical indicator suspicious for invasive cervical cancer.
In practice, women with a VIA screening (or triage) test result of “positive” or “suspected cancer” are both considered screen-positive (or triage-positive); however, for the purposes of monitoring, screen-positive results are separated into precancerous lesions (“positive” disaggregate) and suspected cancer (“suspected cancer” disaggregate) because the care pathways for each are different. Precancerous lesions may be treated immediately with outpatient procedures, whereas suspected cancer requires further evaluation (colposcopy, biopsy, diagnosis) before treatment options can be considered. Clinical definitions can be found in Comprehensive cervical cancer control: a guide to essential practice [WHO, 2014].
Screening visit type
- 1st time screening
- This disaggregate allows the monitoring of screening service provision (and positivity rate) in the screening-naïve HIV-positive population – only women being screened for the first time in their lifetime should be counted under this disaggregate
- Rescreening after previous negative result
- This disaggregate allows the monitoring of screening service provision (and positivity rate) in the population of HIV-positive women who have received at least one cervical cancer screening test in their lifetime, and who received a negative result on their most recent screening test
- WHO recommends that HIV-positive women or women of unknown HIV status who receive a negative cervical cancer screening test result be rescreened every 3 years; however, the results of PEPFAR modeling exercises led to the current PEPFAR recommendation of a screening interval (for women with a negative result) of every 2 years for HIV positive women?
- As a program matures, countries should consider adding an additional performance indicator which measures whether women that should return for routine rescreening in a given time period are returning in that time period (e.g., number of rescreened women in a given time period, over the number of women who were expected to be rescreened in the same time period)
- Post-treatment follow-up screening
- This disaggregate allows the monitoring of screening service provision (and positivity rate) in the population of HIV-positive women who have received at least one cervical cancer screening test in their lifetime, and who received precancerous lesion treatment due to a positive screening result on their last screening test
- Some national guidelines require post-treatment follow-up screening at intervals other than or in addition to 1 year (e.g., 6 months and 12 months) – programs should use additional indicators to monitor the additional follow-up time points, and this should be noted in the narrative.
The numerator captures the number of individual HIV-positive women on ART who received a screening test for cervical cancer.
See TX_CURR for more details.
Indicator changes (MER 2.0 v2.3 to v2.4): None
PEPFAR-support definition:
Standard definition of DSD and TA-SDI used.
For cervical cancer screening services, direct service delivery includes: ongoing procurement of critical screening related commodities or requisite materials such as specula, acetic acid, bright white light source (bulbs/lamp, or torch/batteries), or other consumables (cotton swabs, exam gloves, gauze, etc.), or funding for salaries of screening service providers including program managers, supervisors, and/or coordinators. Staff who are responsible for the completeness and quality of routine patient records (paper or electronic) can be counted here; however, staff who exclusively fulfill MOH and donor reporting requirements cannot be counted.
For cervical cancer screening services, ongoing support for service delivery improvement includes: clinical mentoring/supportive supervision, VIA training, guidance development, infrastructure/renovation of facilities, site level QI/QA, routine support of M&E and reporting, or commodities consumption forecasting and supply management.
Guiding narrative questions:
- Are there any barriers you face encouraging HIV-positive women on ART to get screened for cervical cancer and, if so, what would be helpful to overcome these barriers?
- Please provide the context for how real-time (or near real-time) imaging technologies are in use at your sites. For instance, do you have the option to send images to a central location for review? If so, do they provide feedback while the client is still at your site or does the delay in processing necessitate a return visit for the client?
- For areas where VIA is not the preferred screening test (i.e., where HPV testing or Pap smear are more common), describe the challenges in promoting and scaling up this option.
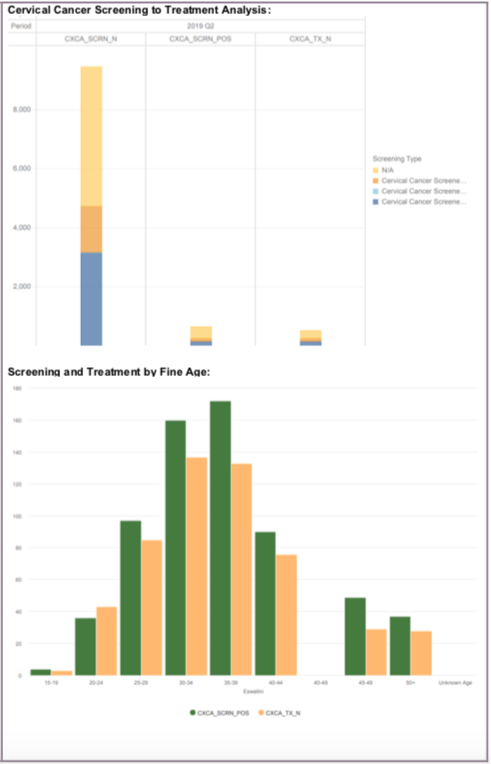
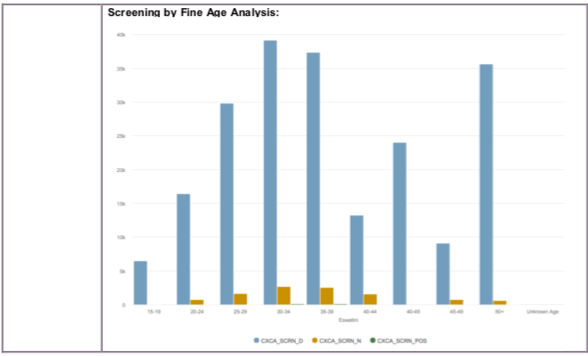
Data Visualization and Use Examples:
Related Indicators
ST.3 Cervical cancer screening among women living with HIV, 2020, WHO Consolidated HIV strategic information guidelines: driving impact through programme monitoring and management (https://www.who.int/publications/i/item/consolidated-hiv-strategic-information-guidelines).
10.8 Cervical cancer screening among women living with HIV, Global AIDS Monitoring 2020: Indicators for monitoring the 2016 Political Declaration on Ending AIDS (https://www.unaids.org/sites/default/files/media_asset/global-aids-monitoring_en.pdf).